
Translate this page into:
Biologic restoration: A successful treatment option for immediate esthetics – A case report

*Corresponding author: Deep Shah, Department of Conservative Dentistry and Endodontics, Coorg Institute of Dental Sciences, Virajpet, Karnataka, India. sdeep92@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Shah D, Ponnappa KC, Subbaiah N, Ponappa MC. Biologic restoration: A successful treatment option for immediate esthetics – A case report. J Restor Dent Endod 2021;1(1):17-22.
Abstract
Crown fractures mainly in the anterior region are the most common outcome of traumatic injuries. The common cause is ascribed to falls, motor vehicle accidents, and contact sports. Out of all the dental trauma injuries, dentoalveolar trauma contributes to about 25%, which may vary from simple crown fracture of enamel and/or dentin to complicated crown root fractures. In this case report, an undergraduate dental student reported with a fractured crown due to a fall an hour earlier. The clinical and radiographic assessment leads to the diagnosis of an uncomplicated crown fracture. Fracture line was extending obliquely till the middle third of the crown involving enamel and dentin. Tooth segment adaptation was evaluated, and decision was made to attempt for reattachment procedure. The tooth was isolated using rubber dam and tooth fragment was reattached using flowable composite. Follow up period was noted for 6 months. Tooth segment reattachment is a minimally invasive procedure with immediate aesthetic and it is not time consuming. This procedure has a predicable long-term prognosis with minimal complication due to advances in adhesive technique. Various factors should be taken into consideration for maximizing the benefits. Thus, this simple procedure is an alternative to the other complex restorative procedure for restoring tooth function, form, and esthetics. Recent advances in flowable composites can be used for a much more predictable result pertaining to strength and aesthetics.
Keywords
Traumatized central incisor
Composite resin
Tooth fragment reattachment
Traumatic injury

INTRODUCTION
Crown fractures mainly in the anterior region are the most common outcome of traumatic injuries. The etiology can be ascribed to falls, motor vehicle accidents, and contact sports.[1] Out of all the dental trauma injuries, dentoalveolar trauma contributes to about 25%, which may vary from simple crown fracture of enamel and/or dentin to complicated crown root fractures.[2] Retaining the original tooth segment and its usage for restoring the tooth form and shape can provide better and immediate esthetics, improved function. It also precludes the patient from psychological stress of tooth loss without having to undergo major procedures.
This paper reports successful treatment of an uncomplicated tooth fracture using adhesive reattachment technique.[3]
CASE REPORT
An undergraduate dental student reported with a fractured crown due to a fall an hour earlier.
She gave no history of previous restoration to the same tooth. The tooth segment was brought stored in distilled water.
Fracture line was extending obliquely up to the middle third of the crown involving enamel and dentin. No intraand extra-oral soft-tissue injuries were noted. Periodontal apparatus was in good physical condition without any mobility.
Pulp sensibility tests were performed for the baseline value assessment of the pulp status using an ice stick. Similarly, it was assessed for adjacent teeth also periapical radiographs were assessed to rule out any root fracture. Subsequently, follow-up was done for 4 weeks to note for any degenerative changes in the pulp.
The clinical and radiographic assessment steered the diagnosis toward an uncomplicated crown fracture. Tooth segment adaptation was evaluated, and decision was made to attempt for reattachment procedure
The prognosis of the reattachment was appraised based on the following parameters: Patient’s esthetic concern, age of the patient, sound adaptation of fractured tooth segment, and the health of the periodontium. The patient was explained about the procedure and written consent was obtained.
Before start of reattachment procedure, oral prophylaxis was done. Tooth segment was disinfected using 2% CHX (STEDMAN Pharmaceutical Pvt. Ltd.). Before the commencement of reattachment procedure, short bevel was placed along the margins of the tooth segment and the tooth portion with a thin tapered diamond point (Dia-burs Mani, Japan).
The tooth was isolated using rubber dam, as improper isolation affects bonding. The tooth remnant and the fragment were etched with 37% phosphoric acid (Scotchbond Multi-purpose etchant, 3M ESPE, USA) for 20 s followed by washing with air/water spray and subsequent drying. Then, a conventional 5th generation adhesive system (Scotchbond Multi-Purpose Plus, 3M ESPE, USA) was applied over the fragments and cured.
Flowable microfilled composite was placed on the tooth surface and tooth fragment was placed back, firm pressure was applied to improve the adaptation and was light cured for 40 s each on labial and palatal aspects. Excess flowable composite was removed before polymerization [Figure 1].

- Intraoperative procedure.
The patient was advised to avoid any excess occlusal loading.
Clinical and radiographic assessment of the traumatized tooth was done at 1 and 3 months interval [Figure 2], but no degenerative changes of pulp or periodontium were observed. Attached segment was assessed for color stability and esthetics.
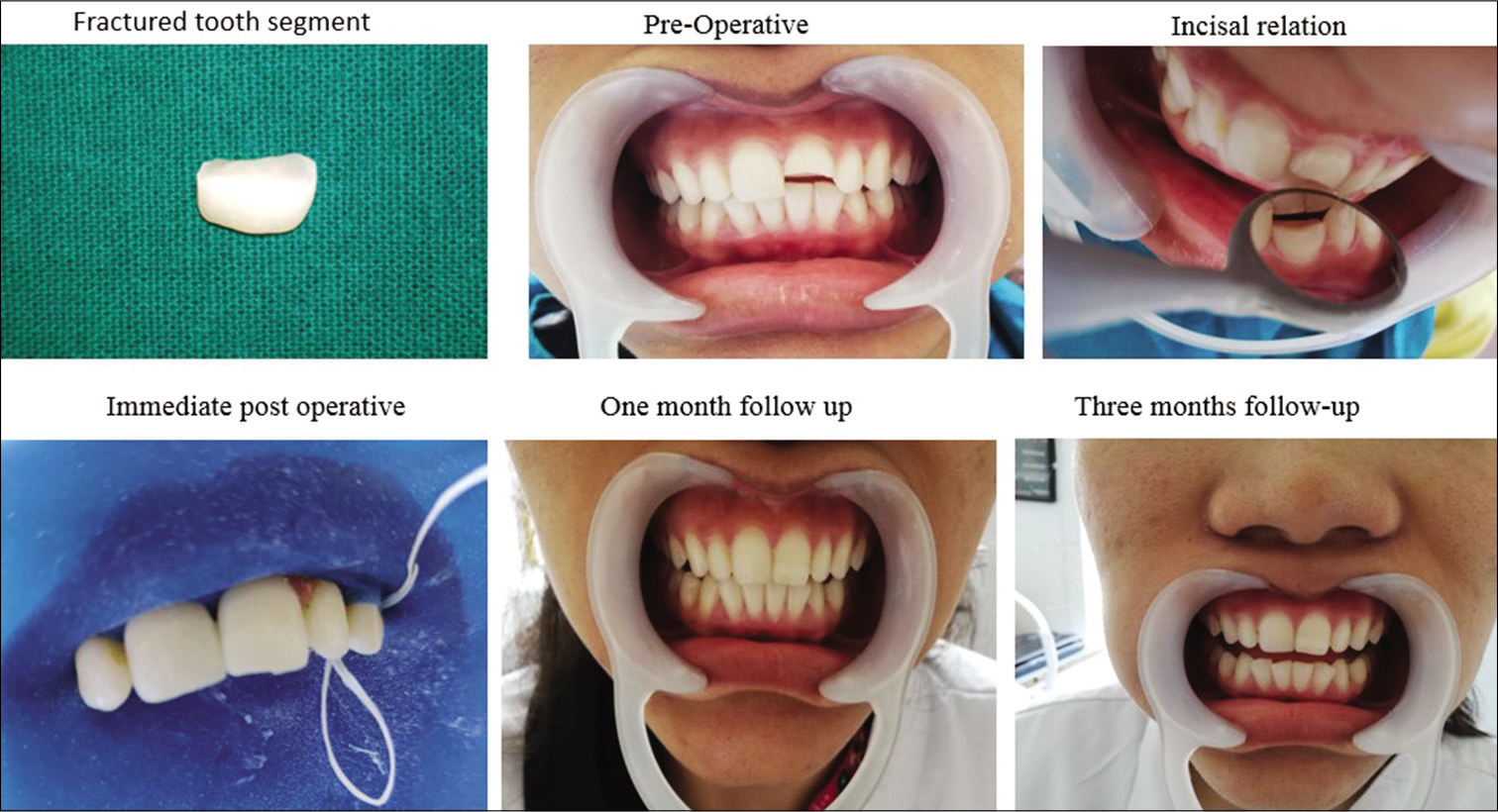
- Pre-operative, follow-up 1 month, 3 months, respectively.
During the follow-up period, slight color change of tooth fragment was noted, but without causing any esthetic concern. Clinical and radiographic assessment revealed healthy pulp and periodontium at subsequent follow-up visit at 1 and 3 months.
Outcome
The patient was asymptomatic following reattachment and is under appropriate follow-up since she is an UG student. Even though slight color change of the fragment was noted during follow-up period, tooth maintained its esthetics, structure, and functionality.
DISCUSSION
The newer advancement in adhesive dentistry and flowable resin composites has made reattachment of tooth segment a procedure with predictable restorative outcome, offering a favorable prognosis. However, this technique is limited to use of only intact tooth fragment and when occlusal forces are within physiological limits.[3] Advantages of tooth fragment reattachment are an immediate esthetically pleasing result, with a perfect shade and translucency match. This technique prevents the patient from the psychological stress of losing tooth, and good clinical satisfaction is achieved due to rerestoration of natural tooth contour and contacts. Tooth segment attachment is an economical option along with immediate esthetic. In the past, different procedures for retaining the tooth segment on the tooth have been advocated, namely, usage of posts, pins, circumferential external bevel of the enamel, undercut preparations within the pulpal chamber, and creating the notch within the enamel. Reports suggest no uniformities in any particular procedure having a better prognosis than the other.[4]
In the present case, an ultraconservative approach was adopted and the fractured fragments were reattached.
Soon after the trauma, it is advisable to keep the tooth segment hydrated outside the mouth for maintaining natural esthetics and to ensure sufficient bond strength. In the present case, the fractured fragment was preserved in distilled water until reattachment, it improved the esthetics with proper color matching to the natural tooth structure. Biological restoration is minimally invasive procedure for restoring the tooth function and esthetics with minimal sacrifice of the remaining tooth structure.[5]
Few limitations of tooth fragment reattachment are compromised esthetics in dehydrated tooth segment and discoloration of fracture tooth segment overtime. Such cases require monitoring for a longer period due to failure in the bonded junction since its progressive breakdown leads to separation of tooth segment.
There is no unanimity in the published data concerning the type of marginal preparation and the long-term efficiency in the reinforcement of the tooth after fractured segment reattachment. It has been observed that, beveling enamel surface enhance strength of the tooth, when equated to direct adhesion devoid of any type of preparation.[6] However, any of these procedure can only reinforce the tooth to certain extend without reaching the initial tooth strength of normal tooth present. Thus, incisal loading is not preferred due to lack of strength.[5]
There is a constant increase in the esthetic demand among the general population and loss of anterior tooth causes huge impact on person’s well-being, self-esteem, and confidence. Any delay in the restoration of anterior impacts daily routine and has negative psychological effects. Thus, in the present case report, the patient being a dental student had high esthetic demand and concern of peer pressure was factored, hence, option of getting it restored with minimal intervention was considered.[7,8]
Survival rate varies due to many factors [Tables 1 and 2].[12-21] According to different studies, Andreasen et al.[9] in their clinical follow-up of 334 reattached fractured incisors reported 50% and 25% retention after 5 and 7 years, respectively. Another study by Vijayakumaran[10] that investigated 50 reattached incisor fragments over 5 years showed 80% survival rate. The survival rate in patients treated with biological method of tooth reattachment was reported by Sarapultseva and Sarapultseva[11] to be 88.9%
| Author | Year of publication | Factors | Remarks |
|---|---|---|---|
| Andreasen et al. | 1995 | Enamel bonding and enamel dentin bonding | Final retention rate of fragment bonding was similar in the two groups, it took the dentinal bonding group almost 3 times as long to drop to 50% fragment retention. This difference could be attributed to greater bonding strength in the dentinal bonding group |
| Shirani | 2011 | Storage media –normal saline, water, milk, saliva, and dry environments for 24 h | Keeping the fractured parts in milk and saliva environments can increase the required force for fracturing teeth more than the other environments |
| Bruschi-Alonso et al. | 2010 | Effect of materials and techniques on impact strength –reattachment technique (direct bonding or circumferential chamfer); the adhesive system (Single Bond or Clearfil SE Bond); and the intermediated material (Filtek Z350 Flow or Rely X CRA) | No technique or material, when individually considered, was capable of achieving the mechanical strength of the sound teeth However, the association of reattachment technique circumferential chamfer with bonding system single bond could approximate the immediate impact strength of the restored teeth to that observed in the sound teeth |
| Liu | 2002 | The effects of surface treatment and joint shape on bond strength of reattached root dentin segments | Significantly higher bond strengths were shown for the non-polished and the etched group than for the polished group |
| Krishna et al. | 2015 | Evaluation of adhesive and tooth preparation combinations used in reattachment of fractured teeth: An ex vivo study | Reattachment with resin luting cement and the preparation design of “groove with shoulder” showed better results |
| A Reis | 2001 | (1)Fracture strength using differenttechniques – bonded only = just bondingthe fragment; (2) chamfer group = afterbonding, a chamfer was prepared on theenamel at the bonding line and filled withcomposite; (3) overcontour group = afterbonding, a thin composite overcontour wasapplied on the buccal surface around thefracture line; (4) internal dentinal groove= before bonding, an internal groove wasmade and filled with a resin composite;(5)resin composite group = after a bevelpreparation on the enamel edge, theadhesive system was applied and thefractured part of the teeth rebuilt by resincomposite? | Reattachment techniques used in Groups 3 and 4, as well as the composite restored group (Group 5), were statistically similar and reached the highest fracture resistance, similar to the fracture resistance of sound teeth. |
| Author | Year of publication | Factors | Remarks |
|---|---|---|---|
| Abdulkhayum et al. | 2014 | In vitro evaluation of fracture strength recovery of reattached anterior fractured tooth fragment using different reattachment technique – simple reattachment, external chamfer, overcontoured, and internal dentinal groove | Internal dentinal groove and overcontoured technique recovered maximum fracture strength than other methods |
| Poubel et al. | 2017 | Effect of dehydration and rehydration | Rehydrating a tooth fragment for 15 min before bonding with a multimode adhesive maintained sufficient moisture to increase reattachment strength |
| Madhubala | 2019 | Effect of two rehydration technique –distil water 15 min, humidificationchamber for 15 min | Fracture resistance after fragment reattachment was significantly affected by the rehydration of fragments for 15 min in the humidification chamber |
| Shirani | 2013 | Preservation of coronal tooth fragments before reattachment – distilled water, milk, egg white, or 50% dextrose solution for 2 h | Preservation of the fractured tooth fragment in egg white or hypertonic solutions results in a higher strength of the bond between the restoration and the tooth as compared to storage in water or dried conditions |
| DM, Ajayi (a systematic review) | 2018 | SURVIVAL OF REATTACHED TOOTH – using different composite material | Follow-up of cases of tooth fragment reattachment which ranged from 3 months to 10 years to monitor the color stability, fracture resistance, and survival rate |
In this case report, the fragment was well adapted, so we opted for the use of flowable microfilled composite along with a short bevel to achieve thorough hybridization of the dental tissue.
CONCLUSION
Tooth segment attachment is a minimally invasive procedure with immediate esthetic and it’s not time consuming. This procedure has a predictable long-term prognosis with minimal complication due to advances in adhesive technique. Various factors should be taken into consideration for maximizing the benefits. Thus, this simple procedure is an alternative to the other complex restorative procedure for restoring tooth function, form, and esthetics.
Recent advances in flowable composites can be used for a much more predictable result pertaining to strength and esthetics.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Tooth fragment reattachment: A case report. Oper Dent. 2015;40:227-34.
- [CrossRef] [PubMed] [Google Scholar]
- Dental Trauma Guidelines San Diego, California: The International Association of Dental Traumatology; 2017.
- [Google Scholar]
- Crown fractures In: Andreasen FM, Andreasen JO, Anderson L, eds. Textbook and Color Atlas of Traumatic Injuries to the Teeth (4th ed). Oxford: Blackwell Publishing Ltd; 2007. p. :280-313.
- [Google Scholar]
- A case report of uncomplicated crown fracture: Tooth fragment reattachment. Br Dent J. 2019;227:259-63.
- [CrossRef] [PubMed] [Google Scholar]
- Factors influencing repair of dental restorations with resin composite. Clin Cosmet Investig Dent. 2014;6:81-7.
- [CrossRef] [PubMed] [Google Scholar]
- Reattachment of dental fragments-an immediate esthetic alternative. J Indian Acad Aesthet Cosmet Dent. 2010;7:29-33.
- [Google Scholar]
- Impacts of missing upper anterior teeth on daily living. Int Dent J. 2009;59:127-32.
- [Google Scholar]
- The psychosocial impacts of implantation on the dental aesthetics of missing anterior teeth patients. Br Dent J. 2012;213:E20.
- [CrossRef] [PubMed] [Google Scholar]
- Long-term survival of fragment bonding in the treatment of fractured crowns: A multicenter clinical study. Quintessence Int. 1995;26:669-81.
- [Google Scholar]
- Evaluation of crown restoration of fractured anterior teeth using original tooth fragment. J Dent Res. 1998;77:696.
- [Google Scholar]
- Long-term results of crown fragment reattachment techniques for fractured anterior teeth: A retrospective case-control study. J Esthet Restor Dent. 2019;31:290-4.
- [CrossRef] [PubMed] [Google Scholar]
- Effect of storage environment on the bond strength of reattachment of crown fragments to fractured teeth. J Conserv Dent. 2011;14:269-72.
- [CrossRef] [PubMed] [Google Scholar]
- Reattachment of anterior fractured teeth: effect of materials and techniques on impact strength. Dent Traumatol. 2010;26:315-22.
- [CrossRef] [PubMed] [Google Scholar]
- Effects of surface treatment and joint shape on microtensile bond strength of reattached root dentin segments. J Prosthet Dent. 2004;91:46-54.
- [CrossRef] [PubMed] [Google Scholar]
- Shear bond strength evaluation of adhesive and tooth preparation combinations used in reattachment of fractured teeth: an ex-vivo study. J Indian Soc Pedod Prev Dent. 2015;33:40-3.
- [CrossRef] [PubMed] [Google Scholar]
- Re-attachment of anterior fractured teeth: fracture strength using different techniques. Oper Dent. 2001;26:287-94.
- [Google Scholar]
- In-vitro evaluation of fracture strength recovery of reattached anterior fractured tooth fragment using different re-attachment techniques. J Clin Diagn Res. 2014;8:208-11.
- [CrossRef] [PubMed] [Google Scholar]
- Effect of dehydration and rehydration intervals on fracture resistance of reattached tooth fragments using a multimode adhesive. Dent Traumatol. 2017;33:451-7.
- [CrossRef] [PubMed] [Google Scholar]
- Comparative evaluation of fracture resistance using two rehydration protocols for fragment reattachment in uncomplicated crown fractures. Dent Traumatol. 2019;35:199-203.
- [CrossRef] [PubMed] [Google Scholar]
- Preservation of coronal tooth fragments prior to reattachment. Aust Dent J. 2013;58:321-5.
- [CrossRef] [PubMed] [Google Scholar]
- Survival of reattached tooth: A systematic review. J West Afr Coll Surg. 2018;8:59-84.
- [Google Scholar]




