
Translate this page into:
Effect of caries excavation by Carisolv and SmartPrep burs on dentin hardness — An in vitro study
 , Ashish Shetty1, D. P. Souparnika1
, Ashish Shetty1, D. P. Souparnika1

*Corresponding author: Meenu Elizabeth Saju, Post Graduate Student, Department of Conservative Dentistry and Endodontics, Bangalore Institute of Dental Sciences and Hospital, Bengaluru, Karnataka, India. meenuelizabethsaju@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Mohan I, Saju ME, Julia A, Raghu R, Shetty A, Souparnika DP. Effect of caries excavation by Carisolv and SmartPrep burs on dentin hardness — An in vitro study. J Restor Dent Endod 2021;1:53-8.
Abstract
Objective:
The purpose of this study was to comparatively evaluate two caries excavation methods-Smartprep(SS White) burs and Carisolv (Carisolv™) by measuring the Vickers hardness of prepared cavity.
Materials and Methods:
40 extracted human molars with moderate occlusal caries were used in this study. Teeth with moderate caries extending till dentin without pulp involvement were selected. RVG was used to assess the depth of the cavity. The samples were divided into 2 groups, Group I by Smart prep burs and Group II using Carisolv. Each groups were subjected to morphological analysis under scanning electron microscope.
Results:
The samples prepared with Carisolv showed least difference in hardness values between the prepared surface and surrounding dentin compared to Smartprep burs. SEM analysis with Smartprep burs revealed surface covered with debris and smear layer while Carisolv showed rough and scaly surface with large areas with open dentinal tubules.
Conclusion:
Removal of infected carious dentin was superior when Carisolv was employed as compared to SmartPrep burs. The results concluded that smear layer removal of Carisolv was superior when compared to SmartPrep burs.
Keywords
SmartPrep bur
Carisolv
Infected dentin
Vickers Hardness test
SEM

INTRODUCTION
Globally, dental caries is the most common non-communicable disease posing a major public health hazard.[1] The advent of adhesive restorative materials coupled with alternative therapeutic approaches has ushered in the era of minimal intervention dentistry. The guiding principle, here, is to “do no harm” as put forward by Hippocrates oath in the field of medicine and dentistry.[3] Keeping in tune with this concept, we are now welcoming “minimal Hazardous Dentistry” that is retaining as much as natural tooth structure as possible.
During the operative treatment of carious dentin, only the superficial layer (infected dentin/soft dentin) which is heavily infected and softened requires removal before restoration placement. The affected layer (firm dentin) is partially demineralized but not contaminated with bacteria. This layer of carious dentin can be remineralized and should be preserved.
Conventionally, a round tungsten carbide bur has been employed to facilitate caries excavation and is one of the most effective methods. However, the problems are as follows: Fear of drill, noise, vibrations, pain, and discomfort while removing carious dentin.[2] Added to that is the possibility of uncontrolled dentin removal due to a lack of tactile feedback.
More patient-friendly minimally invasive approaches like a chemomechanical caries removal (CMCR) method – Carisolv and SmartPrep burs were therefore used in this study.
CMCR is a non-invasive technique of eliminating only the infected dentin through a chemical agent.[4] They chemically dissolve the degraded soft collagen in the infected dentin which can gently be excavated with negligible discomfort to the patient. At the same time, the affected demineralized dentin which is remineralizable, can be safely preserved. It is designed to reduce the need for anesthesia, maintain tooth structure, reduce the use of rotating devices, and effectively relieve anxiety.[5] Specialized hand instruments with permanent or interchangeable tips are used to remove the carious tissue layer by layer. Compared to manual excavation, Carisolv is a promising technique for occlusal caries removal.
The agent that is used in the present study is Carisolv gel which can be applied to the carious lesion and using specially designed hand instruments the soft dentin can be peeled away without causing any pain.
SmartPrep burs are ceramic burs made of polyamide polymer. They are self-limiting in their action, capable of only removing the soft infected dentin. In contact with affected or normal dentin, they lose their cutting efficiency. This bur system is designed to distinguish healthy dentin from carious dentin based on the hardness of sound dentin and was developed to remove decayed dentin without harming healthy tooth structure. It is combined with a specially designed polymer to remove carious dentin without harming healthy tooth structure. The bur’s minute polymer flutes wear away as they come in contact with healthy hard dentin. This self-limiting characteristic helps to ensure that unhealthy dentin is removed carefully.[6]
Hardness tests can serve as objective clinical markers to differentiate between infected, affected, and non-carious dentin. Vickers hardness test is a simple, reliable, and quick method of assessing the hardness of brittle materials like tooth structure. The hardness of dentin might be a useful marker in this respect since the hardness of carious dentin is significantly lower than that of non-carious healthy dentin.
This study aimed to evaluate the efficiency of two different methods of caries removal, namely, chemomechanical methods (Carisolv) and SmartPrep burs by measuring the hardness of remaining dentin after caries removal using Vicker’s indenter. The morphological structure of the cavity floor was also analyzed using a scanning electron microscope.
MATERIALS AND METHODS
Sample preparation
Forty freshly extracted human permanent molars with dental caries were collected from Bangalore Institute of Dental Sciences and Hospital, Bengaluru. About 0.5% sodium hypochlorite was used for initial collection and storage. RVG images of each sample were taken and the extent of dental caries was checked. Samples with moderate dental caries extending beyond the DEJ but without involving pulp were selected. All samples were randomly divided into two groups of 20 each. Group I: Caries excavated with SmartPrep burs Group II: Caries excavated with Carisolv
In both groups, carious dentin was excavated until a clinically “scratchable” cavity surface was attained when tested with a dental probe. After caries excavation, all samples were cross sectioned horizontally, that is, perpendicular to the long axis of the teeth at the occlusal third of the crown and about 1 mm above the prepared surface using a diamond wheel cutter with water. Teeth were then placed in a jig to avoid the movement of the sample during cutting. After sectioning, the cavity surface was flattened and smoothened with sandpaper of 400, 500, and 600 grit in a universal polishing machine. The sections were, then, embedded in a chemically cured acrylic resin with the occlusal surface exposed to the external surface. The blocks were stored in a container filled with distilled water with a few crystals of thymol, immediately at the dough stage of polymerization of the resin to avoid any harm to the dental tissue, as the rise in temperature at this stage is very low. After polymerization of the resin, each block was smoothened further with sandpaper of 400, 500, and 600 grit and kept in distilled water containing thymol 0.1% at room temperature until the hardness measurement was completed.
Measurement of hardness of the cavity floor
Vickers hardness test was used to measure the microhardness of the cavity floor. The testing was performed with diamond pyramid indenters which have a square-based diamond indenter with a 136° angle. The test was then determined using a load of 100 g which was applied to the specimens for 15 s. Measurements were taken using a microscope of ×200.
Scanning electron microscope
After caries excavation, three samples from each group were prepared for scanning electron microscopy. Samples were dried in a critical point drier-based desiccator. SEM images of caries excavated surfaces were obtained. Three microphotographs with different magnifications were obtained for each specimen. The right samples were, then, covered in aluminum foils except for the surface of the cavity floor and mounted on a metal stand coated by gold sputter. Each SEM microphotograph was evaluated and the morphological findings were compared.
RESULTS
Vickers hardness test
The mean Vickers hardness number (VHN) of the surrounding healthy surface using SmartPrep and Carisolv was almost the same [Graph 1], whereas the mean VHN of the prepared surface using Carisolv showed a higher value than the SmartPrep burs [Graph 2]. The difference in mean VHN of the prepared and healthy surface was found to be higher in SmartPrep compared to Carisolv [Graph 3].
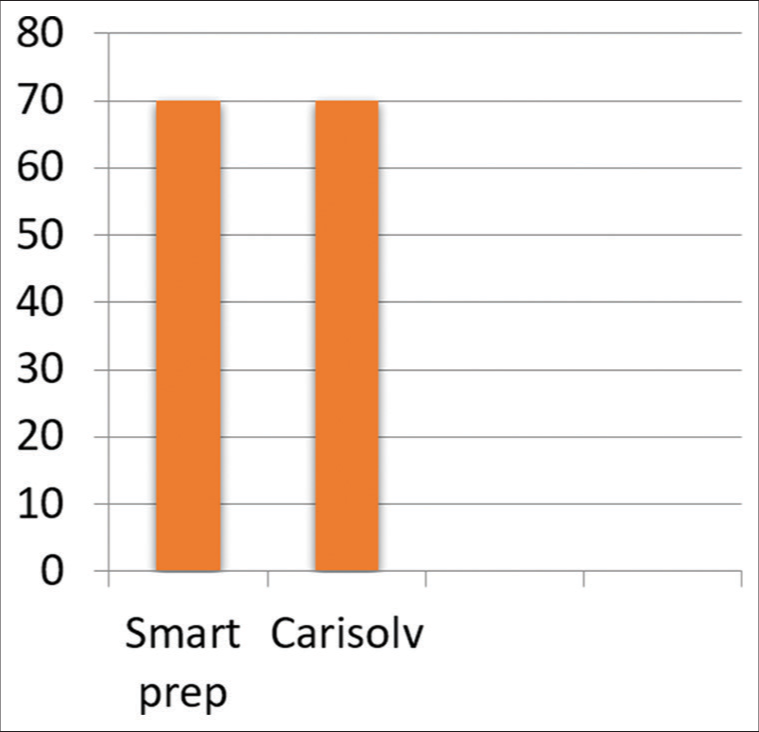
- Mean VNH of the surrounding healthy surface.
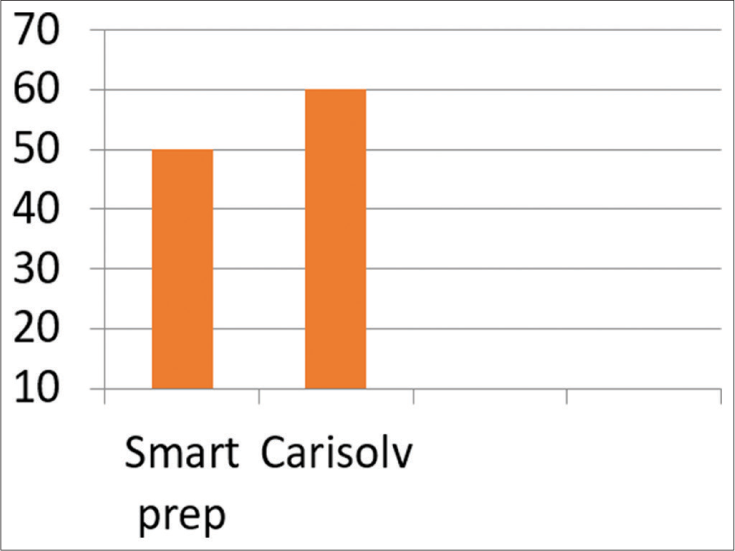
- Mean VNH of the prepared surface.
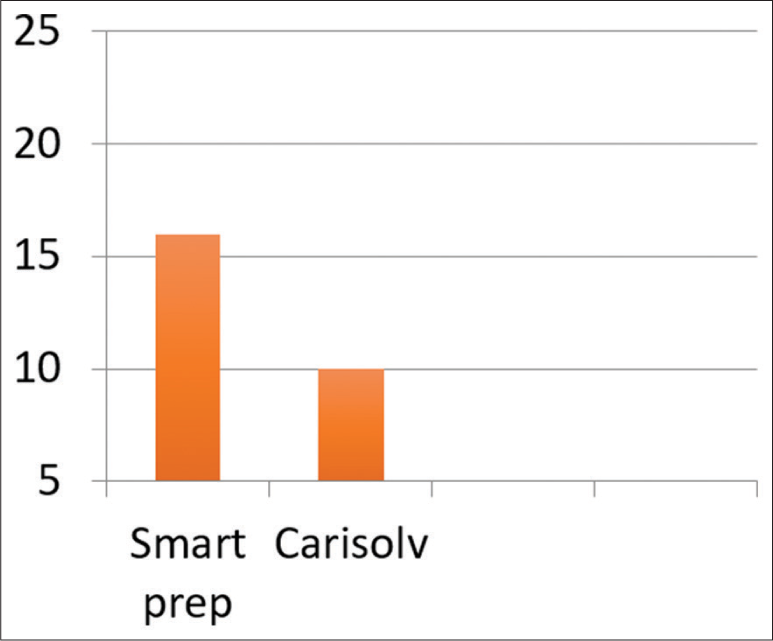
- Mean VNH in the groups for difference in prepared and healthy surfaces.
SEM analysis
After caries excavation three samples from each group were prepared for scanning electron microscopy. Samples were dried in a critical point drier-based desiccator. SEM images of the caries excavated surfaces were obtained. Three microphotographs with different magnifications were obtained for each specimen. The right samples were then covered in aluminium foils except the surface of cavity floor and mounted on a metal stand coated by gold sputter. Each SEM microphotograph was evaluated and the morphological findings were compared.
DISCUSSION
Since the introduction of rotary instruments, operative treatment of carious lesions has resulted in considerable removal of tooth structure which contradicts the new principle of minimal intervention dentistry.[7] To overcome these drawbacks, many alternative methods such as chemomechanical techniques, air abrasion, sono-abrasion, ultrasonic instrumentation, lasers, caries detecting dyes, and polyamide burs have been introduced for caries removal.[8]
Deep dentinal caries consist of two layers each having distinct ultramicroscopic and chemical structures.[9] An alternative method of caries removal selectively removes the infected outer layer of carious dentin which is irreversibly denatured and not remineralizable.[9]
In an attempt to develop a selective caries removal rotary instrument, a “plastic” bur, SmartPrep bur, is made of a medical-grade polymer with slightly lower mechanical properties than sound dentin which has been recently developed.[10] The polymer material has a Knoop hardness number (KHN) of 50 and is designed to have a hardness greater than carious, infected dentin (0–30 KHN) but lower than healthy dentin (70–90 KHN).[2,10]
According to the manufacturer, if the bur touches sound or caries affected dentin, it quickly becomes dull and produces undesirable vibration, making further cutting impossible.[10] Thus, polymer burs are more efficient in treating soft carious lesions while retaining the harder affected dentin. For this reason, the SmartPrep bur has been suggested as it can be used without the need for local anesthesia, increasing patient comfort.[11,12]
CMCR involves the chemical softening of caries dentin followed by its removal by gentle excavation. Carisolv is available as a twin syringe, one containing sodium hypochlorite solution and the other a viscous gel that contains three amino acids: Lysine, leucine, and glutamic acid together with carboxymethylcellulose to make it viscous. Erythrosine dye is added to make it readily visible during use. The contents of the two syringes are mixed immediately before use as their effectiveness begins to fade after 20 min.[13]
The operative steps include application of the solution, scraping off the carious dentin with special excavators, rinsing, and repetition of the procedure until all caries are removed.
Many studies[14,16] have shown that this method is more accepted by pediatric patients who responded positively, but its disadvantage is that it takes a longer time than conventional mechanical methods.
Thus, in the present study, the efficacy of these two techniques SmartPrep (SS White, Lakewood, NJ, USA) and Carisolv (Carisolv Mediteam, Savedalen, Sweden) was evaluated. The hardness of remaining dentin after caries removal was measured and compared with that of surrounding dentine using the Vickers hardness test.
Knowledge of the mechanical properties of caries affected dentin is important to help the clinician understand how much a substrate reacts under masticatory loading conditions and help to predict the behavior of the tooth-restoration interface. Hardness is the ability of a material to resist a permanent indentation. The hardness of carious dentin is slightly lower than that of non-carious dentin.[15] Microhardness analysis has been used as a method to assess the loss of minerals in dental tissues because the reduction in hardness value presents a linear relation to mineral loss.[17] Therefore, the hardness of dentin can serve as an objective clinical marker between caries infected, caries affected, and non-carious dentin.
The hardness of human teeth has been determined by a variety of methods out of which Vickers hardness testing was adapted in this study because it is easy and quick and only requires a tiny area of specimen surface for testing. It has been proved that indentation load is crucial for VHN values and that with the lower loads, it is difficult to read the indentation marks. Studies have reported that the use of a load of 100 g gave a clear indentation to be observed under the microscope.[18] Hence, in the present study, a load of 100 g for 15 s was employed for the microhardness test.
According to the results of the present study, it was observed that the mean difference in VHN of healthy dentin and that of a prepared dentin were highest in the SmartPrep group. Since the mean difference is greater for SmartPrep burs, it can be inferred that the hardness of dentin prepared by SmartPrep bur was much less than the surrounding healthy dentin [Graph 3].
According to the results of this study, SmartPrep burs were less effective in removing infected carious dentin studies have reported presence of smear layer on bur -treated teeth.[21] Despite having a negative rake angle, when pressure is applied, the polymer bur starts to abrade and loses its efficiency quickly. Even the soft light brown lesions were not easily removed. It is supported by other researchers.[23]
Carisolv showing a lesser mean difference between prepared and healthy dentin indicates that Carisolv was more reliable for removing infected carious dentin while retaining affected carious dentin [Graph 3]. Gentle hand excavation may provide adequate tactile feedback with controlled carious excavation. This was also noted in the study by Lennon et al.[19]
In the second part of the study, the surface characteristics of these two methods were observed using a scanning electron microscope. The morphological analysis of caries excavation by the SmartPrep burs showed a surface covered with debris and a smear layer. There were no open dentinal tubules [Figure 1].

- SEM analysis using SmartPrep burs.
SEM observation of the dentin surface after using Carisolv revealed a rough scaly surface with large areas of open dentinal tubules. There was almost no smear layer, similar to our findings [Figure 2]. Hossain et al.[22] and Sakoolnamarka et al.[20] reported a minimal smear layer and open dentinal tubules after chemomechanical caries removal with Carisolv™. In contrast, a study by Ajilal et al.[24] revealed a rough and granular dentin surface with partially patent dentinal tubules and a residual smear layer. Given these diverse results, it appears that the CMCR technique is sensitive and shows variability according to the operator.

- SEM analysis using Carisolv.
The results of SEM observation of the present study demonstrated that Carisolv possessed some distinguishing features compared to SmartPrep burs. Carisolv creates surface roughness and structural changes that may be advantageous for adhesive restorations and techniques such as immediate dentin sealing, deep margin elevation, and cavity optimization.
CONCLUSION
Carisolv proved to be superior to SmartPrep burs in conservatively removing the infected carious dentine. Regarding smear layer removal, SmartPrep burs demonstrated more debris and smear layer removal with patent dentinal tubules which can increase the dentin surface receptiveness for an adhesive restoration.
Acknowledgment
The authors would like to thank Indian institute of science(IISC), Bangalore for their assistance with Scanning Electron Microscopic Analysis.
Declaration of patient consent
Institutional Review Board (IRB) permission obtained for the study.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Comparison of papacarie carisolv in effective chemomechanical removal of dental caries-a systematic review. Annals of R. S. C. B. 2021;25:18867-77.
- [Google Scholar]
- Comparative evaluation of BRIX3000, CARIE CARE, and SMART BURS in caries excavation: An in vivo study. J Conserv Dent. 2020;23:163-8.
- [CrossRef] [PubMed] [Google Scholar]
- Minimally invasive intervention for primary caries lesions: Are dentists implementing this concept? Caries Res. 2019;53:204-16.
- [CrossRef] [PubMed] [Google Scholar]
- Chemomechanical caries removal (CMCR) agents: Review and clinical application in primary teeth. J Dent Oral Hyg. 2010;3:34-45.
- [Google Scholar]
- Evaluation of the efficacy of caries removal using papain gel (Brix 3000) and smart preparation bur (in vivo comparative study) J Pharm Sci Res. 2019;11:444-9.
- [Google Scholar]
- Chemical analysis of dentin surfaces after carisolv treatment. J Conserv Dent. 2009;12:118-22.
- [CrossRef] [PubMed] [Google Scholar]
- A comparative study of the clinical efficiency of chemomechanical caries removal using carisolv and papacarie-a papain gel. Indian J Dent Res. 2012;23:697.
- [CrossRef] [PubMed] [Google Scholar]
- Clinical threshold for carious tissue removal. Dent Clin North Am. 2010;54:541-9.
- [CrossRef] [PubMed] [Google Scholar]
- Current concepts and techniques for caries excavation and adhesion to residual dentin. J Adhes Dent. 2011;13:7-22.
- [Google Scholar]
- Efficiency of the polymer bur smartprep compared with conventional tungsten carbide bud bur in dentin caries excavation. J Oper Dent. 2006;31:256-60.
- [CrossRef] [PubMed] [Google Scholar]
- Carisolv: An aid for non invasive dental caries excavation. Int J Sci Res. 2018;7:73.
- [Google Scholar]
- Microhardness and Ca: P ratio of carious and carisolv treated caries-affected dentine using an ultra-micro-indentation system and energy dispersive analysis of x-rays--a pilot study. Aust Dent J. 2005;50:246-50.
- [CrossRef] [PubMed] [Google Scholar]
- Clinical randomized controlled trial of chemomechanical caries removal (Carisolv) Int J Paediatr Dent. 2006;16:161-7.
- [CrossRef] [PubMed] [Google Scholar]
- Nanomechanical properties of hydrated carious human dentin. J Dent Res. 2001;80:1768-71.
- [CrossRef] [PubMed] [Google Scholar]
- Dentine microhardness after different methods for detection and removal of carious dentine tissue. J Appl Oral Sci. 2012;20:449-54.
- [CrossRef] [PubMed] [Google Scholar]
- Efficiency of 4 caries excavation methods compared. Oper Dent. 2006;31:551-5.
- [CrossRef] [PubMed] [Google Scholar]
- Morphological study of demineralized dentine after caries removal using two different methods. Aust Dent J. 2002;47:116-2.
- [CrossRef] [PubMed] [Google Scholar]
- “A scanning electron microscopic comparison between different caries removal techniques for root caries treatment in vitro. J Oral Laser Appl. 2003;3:235-42.
- [Google Scholar]
- Dentinal composition and knoop hardness measurements of cavity floor following carious dentin removal with carisolv. Oper Dent. 2003;28:346-51.
- [Google Scholar]
- Performance of four dentine excavation methods in deciduous teeth. Caries Res. 2006;40:117-23.
- [CrossRef] [PubMed] [Google Scholar]
- Morphological changes in the caries excavated dentin prepared by rotary, Carisolv™ and Er, Cr: YSGG Laser (Biolase™) Instruments: A scanning electron microscopic evaluation. Int J Laser Dent. 2012;2:1-6.
- [CrossRef] [Google Scholar]




